Is The Abdominal Pain Coming From the Abdominal Wall?
a common and often overlooked cause of ongoing abdominal pain
In patients with ongoing, well localised abdominal pain and normal investigations, abdominal wall pain should be actively considered:
- Abdominal wall pain is a common cause of ongoing abdominal pain, particularly when imaging, blood tests, and endoscopy are normal
- Pain is typically well localised, often fingertip pointed, and reproducible on examination
- Symptoms are frequently movement related and may be posture dependent
- Carnett’s sign is helpful when positive but not required for diagnosis
- Normal investigations do not exclude the diagnosis, as the pain arises from somatic structures, not intra abdominal organs
- Early recognition reduces repeat testing and enables targeted management
Abdominal wall pain refers to pain arising from the somatic structures of the abdominal wall, including cutaneous nerves, muscle, fascia, and connective tissue. It does not originate from intra abdominal organs.
In clinical practice, it is a common and benign cause of ongoing abdominal pain. It is frequently overlooked, particularly when routine investigations are normal, and may lead to repeated imaging or endoscopy before the abdominal wall is considered.
Pain is usually well localised and can often be identified by the patient with a single finger. Examination typically reproduces focal tenderness. Symptoms are commonly exacerbated by movement, posture, or activation of the abdominal wall.
Routine investigations are often normal because standard imaging and endoscopy assess intra abdominal organs rather than superficial nerves or muscle. Normal results should prompt reconsideration of the pain source rather than escalation of testing.
Abdominal wall pain is a diagnosis of inclusion based on history and examination. Recognition allows reassurance, reduces unnecessary investigations, and supports targeted management.


Spectrum of abdominal wall pain syndromes
Nerve related
| Anterior cutaneous nerve entrapment syndrome | focal anterior abdominal wall pain from entrapment of terminal cutaneous nerves at the rectus sheath; classically fingertip localised and movement related. |
| Lateral abdominal wall nerve branch irritation | focal lateral abdominal wall pain from irritation of cutaneous nerve branches outside the rectus sheath; Carnett’s sign often negative. |
| Thoracoabdominal nerve entrapment | dermatomal abdominal pain from thoracic nerve irritation, often radiating to flank or back; commonly brief and paroxysmal. |
| Intercostal neuralgia | sharp or stabbing pain along an intercostal nerve distribution; often positional and episodic. |
| Post herpetic neuralgia | persistent neuropathic pain following herpes zoster; may occur without recalled rash. |
| Thoracic radiculopathy T7–T12 | abdominal or flank pain referred from thoracic spinal nerve root irritation; often posture or movement dependent. |
| Post surgical nerve injury or neuroma | localised neuropathic pain at or near prior surgical scars due to nerve injury or abnormal healing. |
Musculoskeletal and fascial
| Myofascial pain syndrome | pain arising from dysfunctional abdominal wall muscle and fascia; often associated with trigger points and postural factors. |
| Abdominal wall trigger points | focal areas of muscle tenderness reproducing the patient’s pain on palpation. |
| Rectus or oblique muscle strain | pain related to muscle injury or overuse, worsened by abdominal wall activation. |
| Chronic muscle spasm or guarding | persistent abdominal wall muscle tension without acute injury, often associated with pain chronicity. |
| Costal margin pain or slipping rib syndrome | pain due to irritation or abnormal mobility of the lower costal cartilages. |
Gynaecological
| Abdominal wall endometriosis | cyclical or persistent abdominal wall pain caused by ectopic endometrial tissue, often near surgical scars. |
Hernia related
| Occult abdominal wall hernias | localised abdominal wall pain due to small or non visible hernias, often exertional. |
| Post hernia repair neuralgia | chronic neuropathic pain following hernia repair, sometimes mesh or nerve related. |


Pain Mechanisms
Despite varied terminology, most cases arise from a limited number of shared mechanisms.
Subtle mechanical nerve irritation
Small thoracoabdominal nerves are vulnerable where they pass through muscle or fascia, run beneath the costal margin, or change direction. Minor biomechanical changes may cause intermittent nerve irritation without structural abnormality.
Repetitive microtrauma
Cumulative low grade stress related to posture, trunk rotation, lifting, coughing, work or play behaviours or sport may sensitise nerves over time, leading to fluctuating or paroxysmal pain.
Remote injury or inflammation
A prior event may cause transient nerve injury that later leaves the nerve vulnerable. Examples include rib fracture or chest wall trauma, abdominal or thoracic surgery including small laparoscopic ports, direct blows or falls, seatbelt injuries, and prior shingles or viral neuritis. Symptoms may arise years after the original event, often without a clear new trigger.
Myofascial and neural interaction
Muscle tension or trigger points may compress or irritate adjacent nerves, explaining overlap between myofascial pain and neural pain and response to physiotherapy or local injection.
Sensitisation over time
Repeated nociceptive input may lead to peripheral and segmental sensitisation, contributing to pain persistence or dermatomal spread. Central sensitisation may develop over time or pre-exist, amplifying pain despite resolution of the original trigger. This explains chronicity, not causation, and does not imply psychological origin.
Diagnostic approach
The diagnosis of abdominal wall pain is primarily clinical. It is based on careful history, precise localisation of pain, and targeted physical examination and at times targeted cutaneous nerve blocks rather than extensive investigation. Imaging and endoscopy are frequently normal because the pain arises from somatic structures of the abdominal wall, not intra abdominal organs.
Key clinical features supporting an abdominal wall source include well localised pain, reproducible focal tenderness, and pain exacerbated by movement or abdominal wall activation.
Typical findings on physical examination
A. Localised trigger point
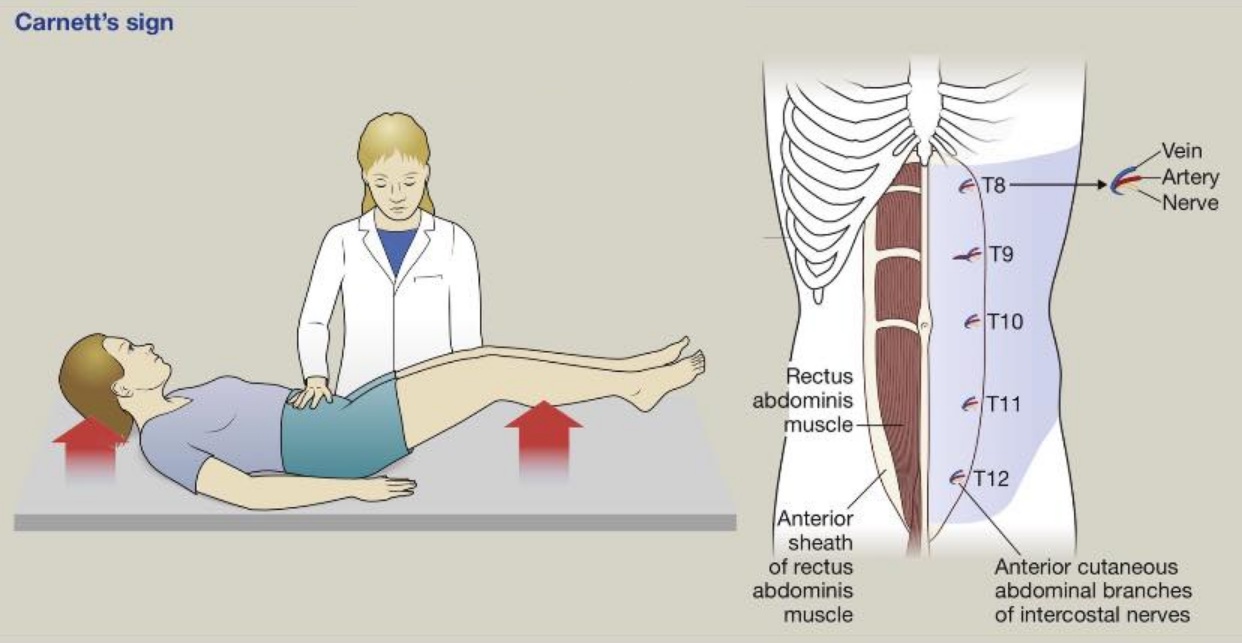
A focal area of maximal tenderness is identified using a single fingertip. Pain typically increases when the abdominal wall is tensed, such as when the patient lifts the head or shoulders during Carnett’s test.
B. Altered cutaneous sensibility
Light touch is assessed using a cotton swab. An area of altered or asymmetric sensation may be detected overlying the pain focus, consistent with involvement of cutaneous nerve branches.
C. Altered thermal sensibility
Cold sensation is assessed using alcohol gauze or a cool swab. Reduced or altered cold perception over the symptomatic area supports a somatic or neuropathic pain mechanism.
D. Pinch test
A fold of skin and subcutaneous tissue is gently pinched between thumb and index finger. Disproportionate pain compared with the contralateral side supports an abdominal wall source.
Carnett’s test and response to local anaesthetic trigger point injection or targeted cutaneous nerve block are useful adjuncts that support, but do not replace, clinical judgement.
Carnett’s sign
Carnett’s sign is supportive when positive but is not sensitive. A negative Carnett’s sign does not exclude abdominal wall pain.
Carnett’s sign increases tension primarily within the anterior abdominal wall, particularly the rectus muscles and anterior sheath. Pain generators that are anterior and mechanically stressed by rectus contraction are most likely to be positive. Pain generators that are lateral, proximal along the nerve course, deep or fascial, or stabilised by contraction may be negative.
Classically Carnett’s positive abdominal wall pain syndromes
These conditions typically worsen with abdominal wall activation because the pain generator lies within or adjacent to the rectus sheath.
-
Anterior cutaneous nerve entrapment syndrome
-
Rectus sheath related nerve entrapment or myofascial pain
-
Painful anterior abdominal wall scar neuroma
-
Anterior abdominal wall endometriosis involving muscle or fascia
Clinical pearl: Carnett’s performs best for midline or para-midline, fingertip localised pain that is present at rest and reproducible on focal palpation.
If Carnett’s sign is negative, can it still be abdominal wall pain?
Yes. Common reasons include the following.
Lateral pain generators outside the rectus sheath
Pain arising lateral to the rectus border may be relatively unaffected by rectus contraction and therefore Carnett’s sign may be negative.
Examples include lateral cutaneous nerve branch irritation, intercostal nerve irritation along the thoracoabdominal course, and oblique or transversus abdominis myofascial pain.
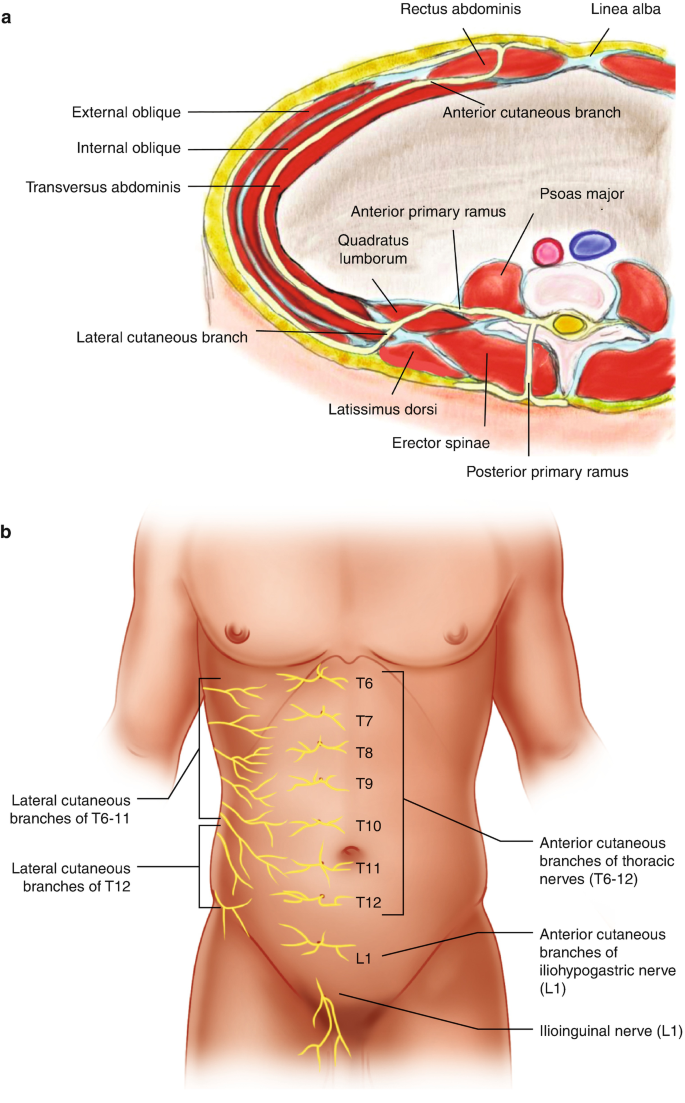
Thoracoabdominal nerves (T6–T12) divide near the lateral border of the rectus abdominis. The anterior cutaneous branches traverse the rectus muscle and pierce the anterior sheath, a common site of entrapment in anterior cutaneous nerve entrapment syndrome. In contrast, lateral cutaneous branches exit the nerve trunk before the rectus muscle and supply the flank and lateral abdominal wall, where pain is less influenced by rectus activation.
Clinical pearl: Para-midline, fingertip-localised pain is more likely to be Carnett’s positive, whereas focal pain just lateral to the rectus border often reflects a cutaneous nerve syndrome despite a negative Carnett’s sign.
Proximal thoracic nerve pathology
If the pain generator lies proximal to the anterior cutaneous branch, abdominal wall activation may not increase mechanical stress at the source.
Examples include thoracic radiculopathy involving T7 to T12, intercostal neuralgia proximal to the anterior cutaneous branch, and post herpetic neuralgia.
Clinical pearl: pain that wraps around to the flank or back, or follows a band-like distribution, supports a thoracic nerve mechanism. Carnett’s may be variable or negative.
Pain improves with stabilisation rather than worsens with tension
In some musculoskeletal and costal margin conditions, abdominal wall activation stabilises the symptomatic structure.
Examples include costal margin pain and slipping rib syndrome, costochondral or costovertebral pain, and rib trauma sequelae.
Clinical pearl: if pain decreases when the trunk is braced, consider rib and costal margin biomechanics rather than excluding an abdominal wall source.
Deep myofascial or fascial tension syndromes
Deep trigger points and fascial pain may not worsen with brief isometric contraction.
Examples include transversus abdominis or internal oblique trigger points, quadratus lumborum referral patterns presenting anteriorly, and fascial tethering following surgery.
Clinical pearl: sustained posture and movement provocation is often more informative than Carnett’s for deep myofascial syndromes.
Intermittent or paroxysmal pain not present during testing
Brief stabbing pains lasting seconds to minutes may not be elicited during examination.
Examples include intercostal neuralgia and thoracoabdominal nerve irritation with ectopic firing.
Clinical pearl: when pain is episodic and investigations are normal, history may outweigh a negative Carnett’s sign.
Scar associated lesions and abdominal wall endometriosis
Pain arising from scar tissue or deep fascia may show variable responses to Carnett’s testing.
Examples include abdominal wall endometriosis, particularly in caesarean scars, and painful scar nodules or fascial tethering.
Clinical pearl: consider abdominal wall endometriosis when pain is focal near a scar and cyclic or period associated. Carnett’s may be positive, negative, or equivocal depending on lesion depth and fixation.
Technique and patient factors
False negatives may occur with imprecise localisation of the tender point, inconsistent pressure, patient guarding, altered muscle recruitment, or inability to adequately tense the abdominal wall.
Clinical pearl: repeat Carnett’s with consistent fingertip pressure, and consider a head lift rather than leg raise when abdominal wall recruitment is limited.
Clinical interpretation for referrers
A positive Carnett’s sign supports an abdominal wall source. A negative Carnett’s sign should prompt consideration of lateral nerve syndromes, proximal thoracic nerve mechanisms, costal margin pathology, deep myofascial pain, or scar associated lesions, rather than exclusion of the diagnosis.
Diagnostic role of local anaesthetic injection
(Insert image: local anaesthetic trigger point or cutaneous nerve block)
A local anaesthetic trigger point injection or targeted cutaneous nerve block can be both diagnostic and therapeutic.
Significant short-term pain relief strongly supports a somatic abdominal wall source, particularly when Carnett’s sign is negative but clinical suspicion remains high. Diagnostic response often differentiates abdominal wall pain from visceral causes and may guide further management.
Clinical pearl: in patients with focal pain and normal investigations, diagnostic response to local anaesthetic is often more informative than imaging.
Why investigations are often normal
Imaging and endoscopy are designed to assess intra abdominal organs and do not detect small nerve or muscle based pain. Normal results indicate that the pain source lies outside the organs being tested.
Management principles
Management is typically conservative and stepwise. It includes clear explanation of the diagnosis, targeted physiotherapy, local anaesthetic with or without steroid injection for diagnostic and therapeutic purposes, and selective use of neuropathic pain agents. Surgical intervention is rarely required.
Clinical message for referrers
In patients with ongoing, well localised abdominal pain and normal investigations, abdominal wall pain should be actively considered before further escalation of testing.