Abdominophrenic Dyssynergia (APD) - Bloating Self Help Guide
Understanding and Self-Managing APD

What is abdomino-phrenic dyssynergia?
Abdomino-phrenic dyssynergia (APD) is a gut–brain coordination disorder that causes bloating and visible abdominal distension. Many people with APD feel uncomfortable fullness or pressure, even when there is little or no excess gas. This page explains what APD is, why it happens, and how doctors diagnose and treat it.
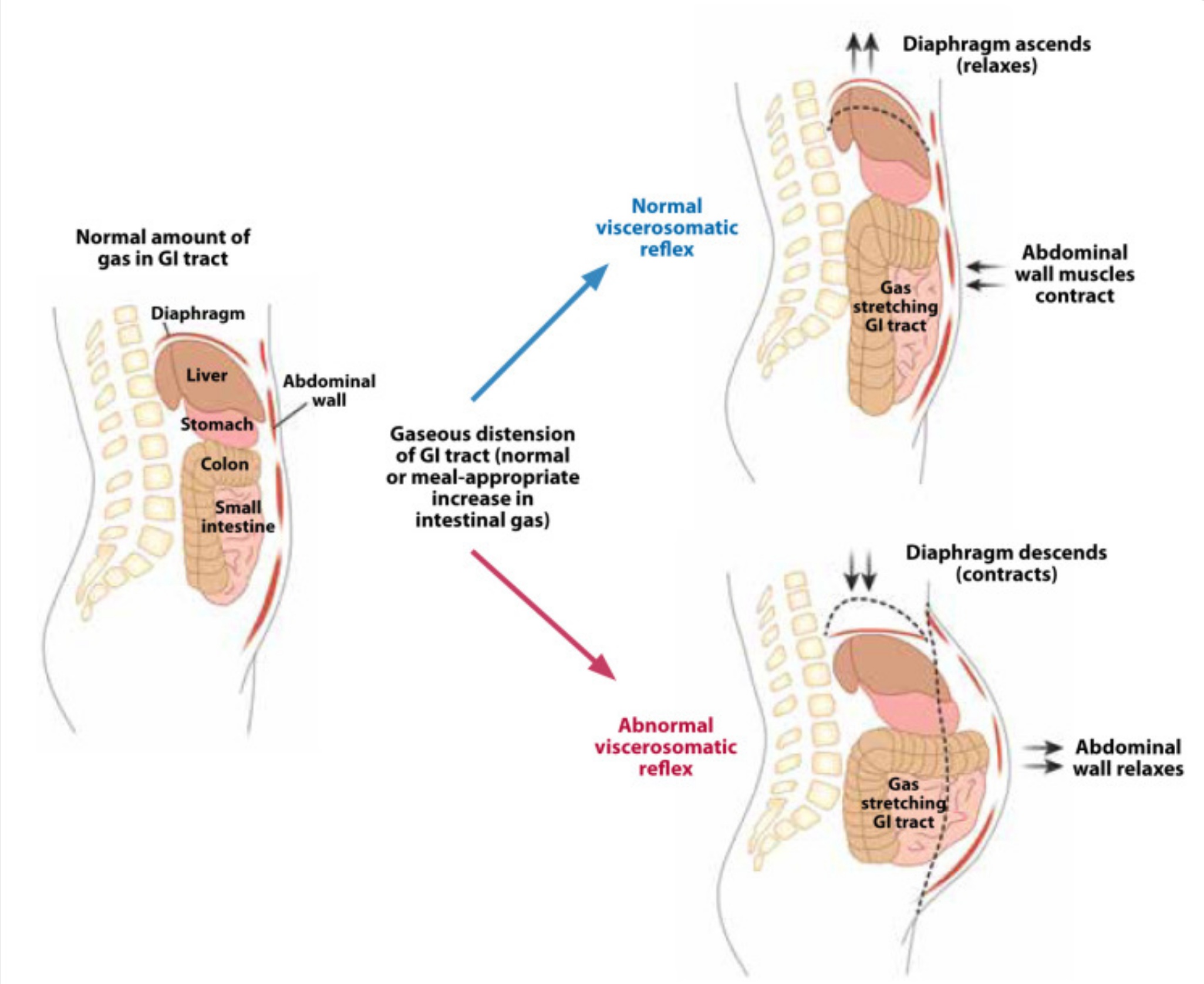
In abdomino-phrenic dyssynergia, the diaphragm contracts and pushes downward at the same time that the abdominal wall relaxes. This pattern is the opposite of what should happen during normal breathing and digestion.
As a result, people with APD may notice:
-
Visible abdominal bloating or distension
-
Tightness or pressure under the ribs
-
A sense of fullness after even small meals
-
Normal test results (such as CT scans, blood tests, or colonoscopy) despite significant symptoms
APD is a real, physical condition. It is not “in your head.” It reflects a problem with timing and coordination between the breathing muscles and the abdominal wall, driven by gut–brain signalling rather than excess gas or structural disease.
Why does it happen?
Abdomino-phrenic dyssynergia (APD) is a common cause of abdominal bloating and visible distension. It reflects abnormal coordination between the diaphragm and the abdominal wall rather than excess gas. APD is usually triggered by a combination of the following factors:
-
Visceral hypersensitivity (the gut becomes more sensitive to normal amounts of gas or volume)
-
Disrupted diaphragm and abdominal wall muscle control
-
Gut–brain signalling changes, often after a gut infection, an IBS flare, stress, or long-standing functional dyspepsia
-
Episodes of constipation or incomplete evacuation
Importantly:
-
APD is not caused by excess gas.
-
The abdominal pressure and abdominal bloating come from muscle mis-activation, not from “trapped wind.”
Common symptoms
People with APD often describe symptoms typical of abdominal bloating and distension, including:
-
A bloated, swollen abdomen that worsens across the day
-
Difficulty fitting clothes by the afternoon
-
Pressure in the upper abdomen or under the ribs
-
Early fullness at meals
-
Breathlessness when the diaphragm is pushed upward
-
Symptoms that improve after lying down or during sleep
-
Often normal bowel motions and normal scans despite significant symptoms
How APD fits into the diagnostic picture
Abdomino-phrenic dyssynergia is a diagnosis based on pattern recognition. Doctors make the diagnosis once serious disease has been considered and excluded, and when symptoms follow a characteristic and reproducible course. APD commonly overlaps with conditions such as IBS, constipation, or functional dyspepsia. The presence of overlap does not weaken the diagnosis.
Other conditions considered but less likely
The following conditions are commonly assessed and actively considered in this context:
Constipation-related bloating
Constipation may contribute to symptoms, but it does not usually account for marked visible distension in the absence of significant stool loading.
Irritable bowel syndrome (IBS)
IBS frequently overlaps with APD. IBS alone, however, does not typically explain pronounced day-progressive distension.
Food intolerance or fermentation sensitivity
Specific foods may trigger symptoms, but APD is driven primarily by abnormal muscle activation rather than gas production.
Small intestinal bacterial overgrowth (SIBO)
This is sometimes considered, although testing has limitations and it does not explain diaphragmatic descent or posture-dependent distension. Sometimes SIBO antibiotic trials over 5-10 days are tested. Effective regimens should cover both aerobic and anaerobic enteric bacteria. The goal is not eradication but modulation of small intestinal microbiota to achieve symptomatic improvement. Clinicians and patients must balance efficacy against risks of long-term broad-spectrum antibiotic therapy, including resistant bacteria, adverse reactions, and Clostridioides difficile infection:
- Rifaximin 400 mg three times daily for 7 days
- ciprofloxacin 500mg bd +/- prokinetic
- Trimethoprim-sulfamethoxazole plus metronidazole (avoid metronidazole monotherapy)
- Amoxicillin-clavulanate 875 mg twice daily for 7 days
- docycyline 100mg daily for 7 days
Repeated courses (e.g., the first 7 days of every month) or continuous therapy with rotating antibiotic regimens to prevent resistance development have been trialed.
Important conditions considered and excluded
These conditions are assessed because they matter, not because they are likely:
-
Inflammatory bowel disease
-
Coeliac disease
-
Ovarian or other abdominal masses
-
Ascites
-
Bowel obstruction
-
Malignancy
Normal investigations make these diagnoses unlikely. This allows management to focus on functional recovery rather than ongoing investigation. Importantly, APD is benign and reversible with appropriate retraining and management.
When APD is the most likely diagnosis
APD is the most likely explanation when:
-
Abdominal bloating or abdominal distension is prominent and often visible
-
Symptoms worsen progressively across the day
-
Routine investigations (blood tests, imaging, endoscopy) are normal
-
There are no alarm features
-
Symptoms improve with breathing retraining, posture adjustment, or targeted physiotherapy
This pattern reflects a disorder of neuromuscular coordination and gut–brain signalling, rather than excess gas, structural disease, anxiety, or imagined symptoms.
How APD is diagnosed in practice
There is currently no single test for APD. Diagnosis is clinical and based on:
-
A typical symptom pattern
-
Normal structural investigations
-
Absence of red flags
-
Improvement with targeted breathing retraining
APD does not require colonoscopy, CT, or blood tests to confirm it. In practice, the most helpful “test” is often a trial of treatment, which is safe, effective, and diagnostic.
Treatment overview
Support from a physiotherapist experienced in gut and breathing disorders can be very helpful. Many people improve with the self-help breathing and posture strategies outlined below. Treatment focuses on retraining coordinated diaphragm and abdominal wall function to reduce abdominal bloating and distension.
1. Diaphragmatic “reset” breathing
Practise twice daily for 5 to 10 minutes:
-
Lie flat or sit upright
-
Place one hand on your upper chest and one on your lower belly
-
Breathe slowly through your nose for 4 seconds, expanding the lower belly
-
Relax your shoulders and upper chest
-
Exhale gently for 6 seconds
-
Aim for the belly to rise while the chest stays quiet
This reduces downward diaphragm pressure and switches off the dyssynergia pattern.
2. Post-meal breathing routine (2 minutes)
After each meal:
-
Sit upright with good lumbar support
-
Breathe slowly into the lower belly
-
Avoid clenching the upper stomach or sucking in the abdomen
-
Let the belt line gently rise with each breath
3. Targeted physiotherapy
Pelvic floor physiotherapists trained in gut disorders, including chronic bloating, pelvic floor dyssynergia, and breathing disorders, can provide:
-
Diaphragm relaxation techniques
-
Abdominal wall strengthening
-
Biofeedback for overactive rib cage breathing
-
Posture correction
4. Gut–brain modulators (if needed)
Low-dose neuromodulators can help reduce visceral hypersensitivity contributing to APD:
-
Amitriptyline 5 to 10 mg at night
-
Mirtazapine 7.5 to 15 mg at night
-
Duloxetine, if anxiety features are prominent
These medicines are non-addictive and work on gut–brain signalling rather than mood.
5. Bowel care
APD often improves when bowel habits are regular:
-
Daily fibre such as psyllium, Metamucil, or partially hydrolysed guar gum
-
Treat constipation early
-
Avoid excessive laxatives, which can worsen abdominal wall relaxation
6. Food triggers
Food rarely causes APD, but large or heavy meals can trigger symptoms because they increase abdominal volume and pressure. Helpful strategies include:
-
Smaller meals
-
Avoiding fizzy drinks
-
Limiting large high-fat meals
-
Eating slowly and chewing well
Low FODMAP diets are usually not needed unless IBS is also present but meals high in FODMAPs can contribute
When to seek medical review
Abdominophrenic dyssynergia (APD) is benign, but you should seek medical review if you experience:
-
Unintentional weight loss
-
Vomiting
-
Persistent diarrhoea
-
Blood in the stools
-
Fevers or night sweats
-
Severe or worsening abdominal pain
These features are not typical of abdominophrenic dyssynergia. They suggest other causes of abdominal bloating or abdominal pain and should be assessed promptly.
Prognosis: does APD get better?
Yes.
Abdominophrenic dyssynergia is highly treatable, and most people improve with a combination of:
-
Diaphragm retraining
-
Posture correction
-
Stress and gut–brain management
-
Physiotherapy
With consistent practice, abdominal bloating and distension usually improve over time. Persistence with exercises is the key.
Self-help summary
- Abdominophrenic dyssynergia is a breathing–abdominal coordination problem, not excess gas
-
Practise diaphragmatic breathing twice daily
-
Do a 2-minute breathing reset after meals
-
Keep bowel habits regular
-
Smaller meals help reduce abdominal bloating
-
Physiotherapy is very effective
-
Neuromodulators may be used to calm gut–brain signalling
-
APD improves over time
APD daily self-help plan
This simple routine helps retrain breathing and abdominal muscle coordination in abdominophrenic dyssynergia and reduce abdominal bloating.
- Morning (before breakfast): 5 minutes diaphragm reset breathing
- After each meal: 2 minutes slow belly breathing + 5–10 minute gentle walk
- During the day: Posture resets (sit/stand tall, ribs relaxed, belly soft)
- Evening: 3 minutes slow breathing (4 seconds in, 8 seconds out) to relax the diaphragm
Consistency beats intensity. Small, regular practice works better than long sessions.
The APD self-help program
A simple 10 to 15 minute daily plan
This program retrains breathing mechanics, strengthens the abdominal wall, reduces diaphragm pressure, and calms gut–brain hypersensitivity that contributes to abdominal bloating and visible distension in abdominophrenic dyssynergia.
1. Morning diaphragm reset (5 minutes)
Do this before breakfast.
How:
-
Sit upright or lie on your back with knees bent
-
Place one hand on your lower belly and one on your upper chest
-
Breathe in through the nose for 4 seconds, letting the belly rise
-
Exhale gently for 6 seconds
-
Keep the shoulders and chest relaxed
-
Repeat 10 to 12 breaths
Why:
This resets diaphragm tone and helps reduce early-day abdominal distension.
2. Post-meal anti-bloat breathing (2 minutes)
Do this after breakfast, lunch, and dinner.
How:
-
Sit with relaxed shoulders and good posture
-
Inhale for 4 seconds and let the belly rise
-
Exhale for 6 seconds and let the belly soften
-
Repeat 8 to 10 cycles
-
Avoid “sucking in” the stomach
Why:
This helps prevent diaphragm descent and abdominal wall relaxation after meals, which contribute to abdominal bloating in abdominophrenic dyssynergia.
3. Post-meal walking (5 to 10 minutes)
One of the most effective strategies
Start 10 to 15 minutes after finishing a meal.
How:
-
Walk slowly and comfortably
-
Keep shoulders down and the rib cage relaxed
-
Prefer nasal breathing if possible
-
Let the belly rise and fall naturally
For more severe APD:
-
Inhale for 2 steps
-
Exhale for 3 steps
Why it works:
Walking helps reset diaphragm position, reduces pressure under the ribs, improves gastric accommodation, and counters the breathing pattern that drives abdominal bloating and distension in abdominophrenic dyssynergia.
4. Rib cage relaxation drill (2 minutes)
How:
-
Place your hands on the lower ribs
-
Inhale and let the ribs widen sideways
-
Exhale and let the ribs soften
-
Keep the shoulders still
-
Repeat 10 breaths
Why:
Upper-chest or rib-dominant breathing tends to worsen abdominophrenic dyssynergia and can aggravate abdominal bloating.
5. Abdominal wall re-engagement (2 minutes)
How:
-
Sit tall
-
Place fingertips just inside your hip bones
-
On the exhale, gently draw the lower abdomen inward using about 10 to 15% effort
-
Hold for 3 seconds
-
Relax
-
Repeat 8 times
Why:
This strengthens the deep abdominal muscles without over-clenching or increasing abdominal pressure.
6. Posture reset (30 seconds, several times per day)
How:
-
Stand or sit tall
-
Lengthen the spine
-
Let the ribs relax downward
-
Keep the belly soft, not held in or pushed out
Why:
Poor posture increases abdominal pressure and can trigger the abdominophrenic dyssynergia pattern and abdominal bloating.
7. Evening diaphragm relaxation (3 minutes)
How:
-
Lie on your back or side
-
Place a warm pack over the upper abdomen or rib area
-
Breathe in for 4 seconds and out for 8 seconds
-
Continue for 3 minutes
Why:
This reduces diaphragm tension before sleep and often improves next-day symptoms of abdominal bloating and distension.
Weekly add-ons
A. Lazy-walk breathing (5 to 10 minutes)
During a slow walk:
-
Inhale for 2 steps
-
Exhale for 3 to 4 steps
-
Focus on belly movement rather than chest lift
B. Gentle core conditioning (2 to 3 times per week)
These help stabilise the abdominal wall:
-
Pelvic tilts
-
Gentle dead bugs
-
Modified bird-dog
Avoid early in recovery:
-
Crunches
-
Planks
-
Heavy lifting
These increase intra-abdominal pressure and can worsen abdominal bloating.
Frequently asked questions
Is this caused by gas?
No. Abdominophrenic dyssynergia is a breathing and abdominal muscle coordination problem, not excess gas.
Does APD improve?
Yes. Most people with abdominophrenic dyssynergia improve significantly with regular exercises, and abdominal bloating usually settles with consistent breathing retraining and posture work.
Is APD dangerous?
No. Abdominophrenic dyssynergia is a benign and reversible condition. It does not damage the bowel or internal organs.
Is medication needed?
Not always. Low-dose gut–brain neuromodulators can help if visceral hypersensitivity is significant, but many people improve without medication.
Do I need to change my diet?
Only if IBS or a food intolerance is also present. Abdominophrenic dyssynergia itself is not a dietary disorder.