Living With Postprandial Distress: Why Tests Look Normal but Symptoms Feel So Real
Your Symptoms Are Real
Postprandial distress syndrome is not “in your head.” It happens because the nerves in your stomach are hypersensitive. Even normal meals can trigger bloating, fullness, or pain. It is within the spectrum of disorders of gut brain interaction. The gut is sometimes called the “second brain”:
- It contains millions of nerve cells, more than the spinal cord.
- These nerves communicate with the brain through neurochemicals like serotonin, dopamine, and noradrenaline.
- In postprandial distress, these signals are turned up too high, so the brain perceives everyday sensations and normal digestion as pain, discomfort, pressure or bloating.
Why the Usual Tests Come Back Normal
Endoscopies and scans are usually normal. That’s because there is no ulcer, tumour, or blockage. The problem isn’t in the structure of the stomach it’s in the wiring and signalling between gut and brain and often it’s the way the nerves interpret normal digestion.
Ways to Picture It
Different explanations make sense for different people. You may find one of these analogies fits best:
- Smoke Alarm → A smoke alarm is meant to protect you. But if it’s too sensitive, even normal cooking steam sets it off. The steam is real, but the alarm is overreacting.
- Car Alarm → A car alarm that blares every time a breeze blows or a cat walks past. The system is working, but it’s misfiring at harmless triggers.
- Sound Amplifier → Imagine a stereo with the volume dial turned up too high. Everyday background noise becomes overwhelming. Medicines can help turn the volume down or work like noise-cancelling headphones.
- Overprotective Security Guard → Like a guard who frisks every guest as if they’re a threat. The gut’s “security system” is jumpy, reacting when it doesn’t need to.
You’re Not Alone: Other Conditions Work the Same Way
This pattern of hypersensitive nerves responding to normal signals isn’t unique to the gut. It happens in other well-recognised conditions:
- Sunburn → When skin is sunburned, even a gentle touch feels painful. In postprandial distress, your stomach nerves act “sunburned,” so normal stretching from food feels uncomfortable.
- Asthma → Airways are twitchy and overreact to dust or cold air. Inhalers calm them down.
- Migraine → The brain’s pain pathways overreact to light, noise, or hormones. Triptans and preventives calm those pathways.
- Fibromyalgia → The body’s pain system is turned up, so normal sensations feel amplified. Treatments aim to turn down that sensitivity.
People with disorders of gut–brain interaction (DGBI) like postprandial distress syndrome, also commonly have overlapping conditions such as endometriosis, interstitial cystitis/bladder pain syndrome, chronic pelvic pain, dysmenorrhoea (painful periods) or dyspareunia (painful sex or intimacy) and overactive bladder. These are recognised under the broader umbrella of chronic overlapping pain conditions (COPCs), which also includes irritable bowel syndrome, fibromyalgia and migraine. Sleep disturbance and fatigue are also common. This overlap doesn’t mean anything dangerous is being missed; it reflects how sensitive nerve systems can affect multiple parts of the body and why a whole-person approach to care helps.
Why Medicines Can Help
Neuromodulators are low-dose medicines used when PPIs or H pylori eradication are ineffective that:
- rebalance gut–brain signalling
- calm down over-sensitive gut nerves
Clinical trials show:
- By 6 weeks, patients often improve more on medicine than on placebo.
- By 8–12 weeks, the placebo group often improves too, narrowing the difference. This is not because the medicine stopped working, but because with time, support, and natural fluctuation symptoms can naturally improve.
Why a Prescription Can Feel Like “Rejection”
Many people feel discouraged when a prescription is offered. Questions often arise:
-
“Does this mean my doctor doesn’t believe me?”
-
“Is this all there is — medicine for life?”
-
“What if something serious has been missed?”
-
“Why is my gastroenterologist giving me an antidepressant? Do they think it’s all in my head or that I am just depressed or anxious?”
The truth is: a prescription is not dismissal. It is one of the few proven ways we have to calm the gut’s alarm system. Neuromodulators at low doses don’t mean the problem is psychological — they adjust nerve sensitivity so normal signals feel normal again.
Some of the medicines we use are also prescribed for patients with depression, anxiety, or epilepsy. This does not mean your symptoms are “all in your head.” Instead, it reflects the fact that the brain and gut share very similar neurochemistry. Over the years, we have discovered that the very same medications that calm overactive brain pathways also calm overactive gut nerves, helping digestion feel normal again. The pathways for relief of digestive pain and discomfort with these engage at much lower doses than those required to treat depression/anxiety (eg. amitriptyline 5-50mg vs 75-300mg).
The goal is not to hand you “a script and nothing more.” You’re using different treatments that change how the gut and brain talk to each other, giving your system the best chance to quieten down and stay that way. Medication is only one part of a whole strategy that you will develop over time with your doctor.
If it feels right, you may meet over a few visits with your specialist or GP to walk this with you, discuss what is and what is not working. They will make adjustments and help fine-tune and reset your gut’s sensitivity, and turn down the alarm systems. This aim is steady, durable improvement, so you can eat, sleep, and live more comfortably again.
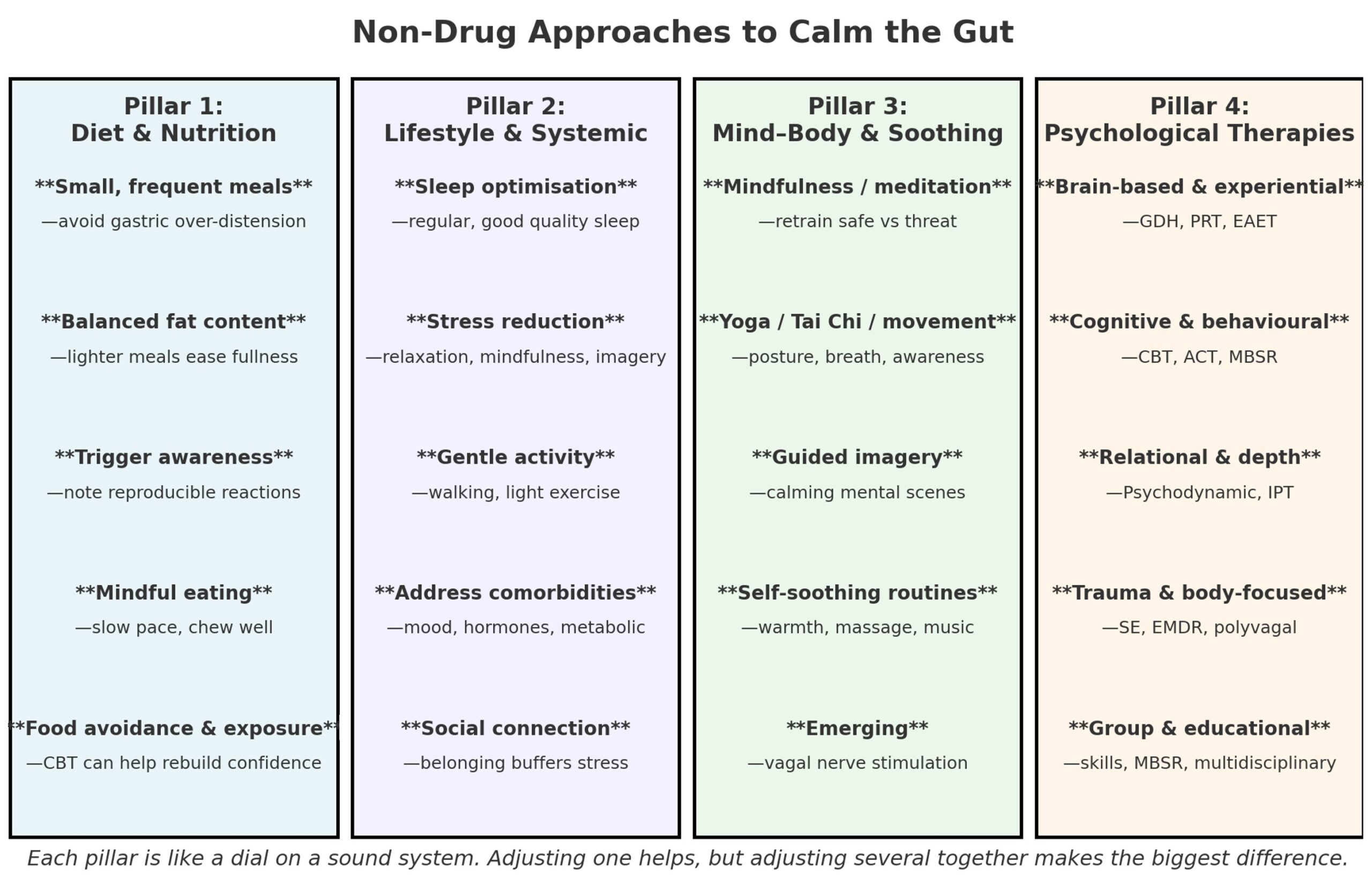
Other Ways to Calm the Gut
Medicines are one tool, but your gut “alarm system” can also be turned down by looking after the whole body, almost like adjusting different dials on a sound system:
- Diet → Balanced meals, avoiding personal triggers (rich, fatty, spicy, high FODMAP or acidic foods), and not skipping meals.
- Physical activity → Regular movement helps gut motility, lowers stress hormones, and supports sleep.
- Sleep → Consistent, refreshing sleep reduces nerve sensitivity and irritability.
- Mental health and stress → Stress and anxiety can turn up the gut’s volume. A therapist can help manage both life stress and the stress of symptoms.
- Connectedness → Support from friends, family, or community improves resilience.
Other health issues → Attending to hormonal balance, mood, or anxiety disorders can reduce background “noise” that otherwise keeps the gut on edge. Sometimes, these are the main disturbance that need attention first.
Diet, Nutrition, and Eating Patterns
Food is one of the most powerful daily signals to the gut, and both what we eat and how we eat can shape symptom intensity. Adjustments in eating patterns often make a noticeable difference, but the picture is rarely one-size-fits-all.
-
Meal size and timing — small, frequent meals help avoid gastric over-distension, which can set off hypersensitive nerves.
-
Fat content — lower-fat meals may reduce impaired gastric accommodation and lessen post-meal heaviness.
-
FODMAPs and fermentables — while most evidence is in IBS, some patients with bloating or PDS find improvement by reducing high-fermentable foods.
-
Trigger awareness — caffeine, alcohol, dairy, gluten, or highly processed foods may provoke reproducible flares. But cultural and individual differences matter: what is “too spicy” in one culture may be a daily staple in another. What matters is reproducibility for the individual, not the food itself.
-
Mindful eating — slowing down, chewing thoroughly, and paying attention to satiety cues reduces swallowed air (aerophagia) and allows the stomach to adapt more smoothly.
Eating is not only biological but also psychological. Many patients develop food-related anxiety or avoidance after repeated unpleasant symptoms. Here, cognitive behavioural therapy (CBT) can help dismantle catastrophic thinking (“this food will always make me worse”) and guide gradual exposure to feared foods or sensations in a safe, structured way. For example, a patient who avoids bread for fear of bloating may be supported to reintroduce small portions, learning that symptoms are tolerable and not dangerous. Over time, this reduces conditioned fear of eating and restores dietary flexibility.
Some patients can experiment with these strategies themselves; others may benefit from working with a dietitian to balance nutrition, or with a psychotherapist to address avoidance and rebuild confidence in eating.
Lifestyle & Systemic Factors
Functional dyspepsia doesn’t sit in isolation from the rest of life. The “volume” of gut symptoms is shaped by whole-body factors — sleep, stress, activity, mood, and even hormonal shifts. Addressing these doesn’t cure the condition, but it reduces the background load on the nervous system, making the gut less reactive day to day.
-
Sleep optimisation — disrupted or insufficient sleep heightens visceral hypersensitivity. Consistent routines, a cool/dark room, and reduced stimulation at night can improve baseline resilience.
-
Stress reduction — stress “turns up” gut reactivity; practices like relaxation training, mindfulness, guided imagery, or structured breaks can buffer flares.
-
Physical activity — gentle post-meal walking or light exercise supports gastric motility and reduces postprandial discomfort.
-
Addressing comorbidities — treating conditions like sleep apnoea, anxiety, depression, or metabolic disorders lowers the load on the nervous system. Hormonal shifts are also relevant: cyclic changes, perimenopause, and postmenopausal low-oestrogen states may heighten gut sensitivity and symptom flares.
-
Social connection — community, relationships, and being listened to provide emotional scaffolding that dampens symptom amplification.
Patients can begin with small adjustments themselves, but input from a sleep specialist, psychologist, physiotherapist, endocrinologist, gynacologist or women's health expert, or GP may help tailor changes. These systemic influences remind us that the gut is not acting alone, it is part of a larger web, and addressing the whole system often makes the stomach easier to live with.
Mind–Body & Soothing Practices
The gut is closely wired to the nervous system, which means practices that calm the body can directly calm digestive sensitivity. These approaches don’t require special equipment and can be integrated into daily routines, creating a gentle background signal of safety.
-
Mindfulness, meditation, or body scan tuning inward with curiosity rather than judgment helps retrain the nervous system to distinguish “safe” from “threat.” Over time, this reduces hypervigilance and the sense that every sensation is dangerous.
-
Yoga, Tai Chi, Alexander technique or gentle movement practices combining posture, breath, and awareness promotes parasympathetic balance, which supports digestion and reduces postprandial distress.
-
Guided imagery or visualisation — imagining soothing internal scenes (warmth, expansiveness, relaxation) shifts gut–brain signalling toward calm.
-
Self-soothing routines — simple comforts such as warm baths, abdominal heat packs, gentle abdominal massage, or calming music help reduce muscular tension and send the body cues of safety.
These practices can be tried independently, but many people find they deepen with support. A mindfulness teacher, yoga or Tai Chi instructor, physiotherapist, or psychotherapist can help integrate these skills more fully. For patients whose symptoms are closely tied to stress or emotional patterns, these practices can be a bridge into more structured psychological therapies that target the brain–gut connection directly.
Psychological therapies
There is a whole ecosystem of psychotherapies for DGBI including PDS/FD. The strongest clinical research evidence is for CBT and gut-directed hypnotherapy, with growing support for PRT and EAET. Long-form psychodynamic work may not have RCTs, but is often transformative for the subset of patients whose GI symptoms are woven into deeper emotional or relational histories. When patients are motivated and open to these approaches, especially if they prefer non-drug options, those with disorders of gut–brain interaction (DGBI) and features of gut hypersensitivity or gut hypervigilance may benefit from:
1. Brain-based / experiential therapies
Gut-directed hypnotherapy (GDH)
Gut-Directed Hypnotherapy
A structured, evidence-based therapy that uses focused attention, deep relaxation, guided imagery and therapeutic suggestions to calm the brain–gut axis. It can reduce gut sensitivity, change symptom focus and improve confidence in managing gut symptoms.
What the evidence shows
Gut-directed hypnotherapy has one of the longest track records among psychological therapies for IBS, with more than 10 randomised controlled trials showing improvement in abdominal pain, bloating, bowel symptoms and quality of life. It also has emerging evidence in functional dyspepsia and postprandial distress syndrome, including improvement in fullness, early satiety and upper abdominal symptoms.
International guidelines recognise gut-directed hypnotherapy as a reasonable option for disorders of gut–brain interaction, particularly when symptoms persist despite standard medical and dietary care. It is generally safe and can be used alongside medicines, dietary strategies and other treatments.
It may be delivered as:
- therapist-guided treatment, preferred when available
- structured self-directed programmes, including audio or app-based programmes, which may help with access and maintenance
Nerva® – Gut-Directed Hypnotherapy for IBS
Nerva is a structured digital gut-directed hypnotherapy programme developed from research led by Simone Peters and collaborators at Monash University. It is primarily designed for IBS and aims to help patients manage symptoms by working on the brain–gut axis.
Clinical studies of digital gut-directed hypnotherapy show meaningful symptom improvement for many patients, although it does not replace individualised medical review where symptoms are severe, changing, or associated with red flags.
Nerva may be recommended as part of a broader management plan alongside education, dietary strategies, physical activity and, where appropriate, medication.
Pain Reprocessing Therapy (PRT)
PRT is a structured psychological treatment designed to reduce the brain’s amplification of pain and the “threat value” of symptoms. First developed for chronic back pain and then fibromyalgia with a landmark research (JAMA Psychiatry, 2021) finding PRT produced dramatic and durable improvements in chronic back pain compared with usual care. With principles overlapping strongly with gut-directed CBT and hypnotherapy, some clinicians have adapted it to gut–brain interaction disorders with good anecdotal results.
PRT draws on neuroscience showing that in many chronic conditions, the brain continues to generate pain or symptom signals long after tissue injury has healed. This is driven by heightened sensitivity and fear-based learning where the nervous system gets “stuck” in protective mode.
Core components include
- Re-framing of symptoms, shifting the story from “something must be broken or damaged” to “my brain is over-protecting me.” Patients can begin to see their symptoms as real but not a sign of ongoing harm.
- safety re-learning, where patients practise experiencing symptoms in safe contexts and reinterpret them as non-dangerous;
- emotional expression and awareness, which involves identifying and processing emotions such as anger, grief, or fear that may keep the nervous system on high alert; and,
- somatic tracking, a mindfulness-based practice of observing bodily sensations with curiosity and calm rather than catastrophising. Together, these practices retrain the brain’s response to symptoms, reducing their intensity and impact over time.
Emotional Awareness and Expression Therapy (EAET)
EAET, sometimes called emotional awareness and reprocessing therapy, is a structured, trauma-informed approach that helps patients become aware of, access, and safely express emotions that may have been suppressed — such as anger, grief, fear, or guilt. It builds on psychodynamic therapy, exposure principles, and modern neuroscience linking emotion and pain. The central idea is that unprocessed or avoided emotions can keep the nervous system in a persistent state of threat and arousal, which in turn maintains pain and bodily symptoms. Evidence includes a landmark RCT in fibromyalgia (JAMA Psychiatry, 2018) showing EAET produced durable improvements in pain, mood, and functioning, with additional studies in chronic pelvic pain and IBS suggesting benefit.
Core techniques include:
-
Emotional education — learning that emotions are biologically protective and safe to feel, and that suppression may “lock” the nervous system in overdrive.
-
Emotional awareness training — noticing subtle bodily cues of emotion and linking them to life events or relationships.
-
Emotional expression — using role-play, imagery, writing, or dialogue to give voice to hidden feelings.
-
Emotional reprocessing — re-experiencing emotions with curiosity and safety rather than avoidance or fear, reducing the conditioned threat response that ties emotions to physical distress.
EAET appears to reduce central sensitisation and enhance emotional regulation. While Pain Reprocessing Therapy (PRT) focuses more on reattributing symptoms to “safe neural circuits” and reducing fear of sensations, EAET leans further into emotional processing. Both approaches aim to retrain the brain’s threat pathways, but through different entry points.
2. Cognitive and behavioural approaches
Cognitive-behavioural therapy (CBT) helps patients reframe and reduce the impact of symptoms by targeting the interplay between thoughts, behaviours, and bodily sensations. It is particularly useful for people who feel preoccupied with symptoms, have symptom-related anxiety, or want to build stress-management skills. Typically delivered in 4–8 sessions, CBT has strong evidence: around 70% of patients achieve meaningful relief with improvements in both symptoms and quality of life. Core techniques include restructuring unhelpful thoughts (for example, “my bloating must mean something is seriously wrong”) and shifting behaviours that maintain distress (such as food avoidance, checking, or hypervigilance). CBT often incorporates relaxation training and behavioural experiments around eating. Patients might be supported to gradually reintroduce feared foods or mindfully experience postprandial sensations, reducing conditioned fear and avoidance over time.
Acceptance-based therapies, including Acceptance and Commitment Therapy (ACT), complement CBT by focusing less on “changing” thoughts and more on changing the relationship to them. Patients learn mindfulness and acceptance strategies to observe uncomfortable sensations or worries without being dominated by them. The aim is to build psychological flexibility: reducing the struggle with symptoms and refocusing on valued life activities. Evidence in IBS and chronic pain shows ACT can reduce symptom interference and improve wellbeing, even when some symptoms persist. Together, CBT and acceptance-based approaches offer practical, skills-based tools for managing functional gut symptoms, reducing distress, and reclaiming quality of life.
3. Psychodynamic and Relational Therapies
Psychodynamic and relational approaches start from a fascinating idea: bodily symptoms often carry unconscious meaning. In other words, the stomach may be “speaking” when words have been suppressed. These meanings are shaped by early relationships, attachment patterns, and unresolved emotional conflicts. Therapy is not only about reducing symptoms but also about helping patients make sense of how distress becomes embodied.
Attachment patterns are the emotional “templates” we form in early life for how safe or unsafe it feels to depend on others. They shape how we respond to stress, relationships, and even physical symptoms:
-
Secure attachment: When care is reliable and nurturing, we grow up able to trust others and share emotions, making stress easier to regulate.
-
Anxious attachment: Inconsistent care can leave us hyper-alert to rejection, amplifying worry and bodily symptoms under stress.
-
Avoidant attachment: Distant care may lead to emotional suppression and self-reliance, with stress showing up in the body.
-
Disorganised attachment: Chaotic or frightening care can create both a longing for closeness and fear of it, keeping the nervous system in “threat mode.”
In therapy, exploring these patterns can reveal how old relational strategies continue to shape present wellbeing. The aim is not to blame childhood but to give patients more freedom now to respond with flexibility, rather than replay automatic patterns.
Short-term psychodynamic psychotherapy (STPP) is a structured, time-limited model (often 12–20 sessions). It helps uncover hidden conflicts and notice patterns that appear in life and in the therapy room. For example, a patient who avoids conflict may also avoid anger in therapy, reporting gut pain instead. Linking these patterns shows how anxiety, attachment, or defences (like suppression or somatisation) can weave into symptoms. RCTs in IBS show STPP outperforms usual care.
Long-form psychodynamic therapy extends this into open-ended exploration, sometimes over months or years. The focus broadens to personality structure, trauma, and identity. For patients with complex histories, gut symptoms may be one chapter in a larger story about loss, self-criticism, or fragile self-worth. Though RCTs are lacking, case series and IBS studies suggest this deeper work can be transformative when symptoms are tied into longstanding struggles.
Interpersonal therapy (IPT), a close cousin, narrows the lens to current relationships, grief, and role transitions. It makes the link between interpersonal strain and symptom intensity explicit. For example, bloating after an argument may be less “coincidence” than a gut response to conflict. IPT offers tools to navigate loss, relationship tension, or major life changes, and has modest evidence for improving distress and gut symptoms.
When to consider: STPP suits patients curious about the emotional meaning of symptoms and open to time-limited work. Long-form psychodynamic therapy fits when trauma, entrenched defences, or identity themes are central. IPT is most relevant when symptoms flare alongside relationship stress, bereavement, or role transitions. None of these approaches dismiss symptoms as “in the head.” Instead, they treat the gut as a messenger of unconscious dynamics — an invitation to explore how the body carries unspoken parts of our story.
4. Trauma-informed and somatic approaches
These therapies start from the premise that trauma and stress are not only psychological events but are also carried in the body. Approaches such as:
- Somatic Experiencing guide patients to tune into subtle bodily sensations, process “stuck” survival responses, and gradually reduce hyperarousal. Small studies in trauma suggest benefits, and while data in gut disorders are limited, the model conceptually fits with visceral hypersensitivity.
- Eye Movement Desensitisation and Reprocessing (EMDR) uses bilateral stimulation (eye movements, tapping, or tones) to help patients safely reprocess traumatic memories. Its strongest evidence is in PTSD, but early reports suggest potential for chronic pain and functional symptoms.
- Polyvagal-informed therapy emphasises that many symptoms reflect shifts in autonomic state rather than organ damage, and works with breath, voice, posture, and social engagement to support vagal tone. While evidence in functional dyspepsia is still conceptual, the framework resonates with patients who experience their symptoms as nervous-system driven.
5. Group, Educational, and Multidisciplinary Models
For many patients, learning itself can be therapeutic.
-
Psychoeducation and skills groups teach the brain–gut model, lifestyle strategies, and relaxation techniques. Group-based interventions in IBS have been shown to reduce distress and healthcare use.
-
Mindfulness-Based Stress Reduction (MBSR) combines meditation, body scanning, and yoga; research in IBS and chronic pain shows reductions in symptom burden and improved quality of life, with limited but encouraging data in FD.
-
Other mind–body practices such as meditation, yoga, or paced breathing can be woven into daily life to regulate the parasympathetic system and calm the gut.
-
Multidisciplinary pain-management programs for those symptoms are severe and disabling bring together medical, psychological, and physical treatments, usually in hospital outpatient settings, to address complex needs in a coordinated way.
No Right or Wrong Order
There isn’t a single “correct” way to approach treatment. Medicines and non-medication strategies can be used in different ways depending on where you are in your journey:
- Sometimes you might choose to work on the non-medication ways first, things like diet, sleep, stress, or working with a therapist through hypnotherapy or “talk therapy.” It might just be one dial turned gently toward healthy. The simple act of starting can be powerful in itself, helping the body move toward healing and relief.
- Other times, it can make sense to start both medicine and lifestyle changes together, giving the best chance of calming the system.
- And sometimes, if you feel overwhelmed, lost, or exhausted after trying many things, it can help to start with a medication trial. By calming the nerves, medicine may create the breathing space also needed to focus on sleep, exercise, or stress management. This is similar to when some overwhelmed by anxiety or depression might sometimes need a medication to “kick-start” brain chemistry before they’re able to benefit fully from “talk therapy”.
You don’t need to feel pressured by the order you choose. Each path is valid and backed up by good scientific evidence, and each complements each other over time.
"I've tried everything and nothing seems to help..."
Some people come after many treatments and feel wary or exhausted. You might notice a pattern of starting something, watching closely for side effects, and stopping early when relief is not clear. If that is you, you are not alone and you are not difficult. You are someone who has been disappointed before and is trying to protect yourself.
A different way to try again
We can treat each option as an experiment rather than a test. No treatment proves anything about you or me, it simply gives us information. We agree on a short window, often four to six weeks, a clear dose plan, and stop rules if side effects outweigh benefits. We measure what matters by using a brief validated symptom scale such as SIBDQ, SF NDI, or IBS SSS before starting and then every two to four weeks, so you can see the trend rather than only the day to day swings. At the end of the trial we ask what changed, what did not, and what we learned, then we either consolidate, adjust, or switch together.
The doctor as a pill
Part of what helps is the relationship itself. My role is not only to prescribe, it is to bring curiosity to your experience so that you can bring curiosity to it as well. When we look at symptoms with calm interest rather than fear, people often discover a little more space, choice, and relief. That exploration is part of the treatment.
If staying with treatment feels hard
Sometimes the wish for a quick fix collides with a problem that needs the longer path. Sometimes any therapeutic relationship can feel unsafe, especially if past experiences have made trust difficult. If that is true for you, we can go more slowly with smaller steps and more check ins. We can add non drug supports such as gut directed hypnotherapy, cognitive behavioural or acceptance based therapies, and simple mind body skills. We can involve people who already feel safe for you, such as your GP, a psychologist, dietitian or nutritionist, a herbalist or naturopath, a personal trainer or physiotherapist, so you are supported by a team.
You always have a choice
If I am not the right fit, or now is not the right time, that is okay. I can write a clear summary for your GP and suggest next steps so you are not starting from scratch. You are not a special case where nothing works, you are a person whose system may need the right timing, the right pace, the right tools, and the right team.
A hopeful roadmap (your timeline may differ)
Think of this as a guide, not a deadline. Many people follow something like this; some are quicker or slower, and that’s okay—we’ll personalise the plan to you.
Week 1–2
-
Hope: better sleep and a little less “gut on edge”.
-
Common: mild nausea or dizziness, some feel a jetlag drowsiness for a few days, when starting a new medicine, usually settles within days.
Week 2–6
-
Hope: pain, fullness/bloating and urgency begin to ease.
-
Daily life often feels more manageable.
Week 6–12
-
We review together.
-
If you’re better, we keep going. If not enough, we adjust the dose or switch to a different, evidence-based option.
3–6 months
-
We consolidate gains.
-
If you remain well, we plan a slow, supervised taper to see if symptoms stay controlled.
It’s normal to have good days and not-so-good days even while improving overall.
If you like numbers: track your progress
Some people find it reassuring to measure how they’re going. If that’s you, ask your doctor for a validated symptom scale so you can see improvement, not just feel it.
-
Examples: SIBDQ (IBD), SF-NDI (functional dyspepsia/PDS), IBS-SSS (IBS).
-
Fill one out before you start, then every 2–4 weeks.
-
Do it at a similar time of day and over the same recall period (e.g., past 2 weeks).
-
Don’t focus on day-to-day swings—watch the overall trend and bring your scores to appointments.
If your timeline is different
-
Slower? We’ll fine-tune the dose, give it a little more time, or try a different neuromodulator or a non-drug therapy (e.g., gut-directed hypnotherapy, CBT, mind–body skills).
-
Faster? Great—we’ll hold steady to lock in progress before tapering.
-
Side-effects? Tell us early; small changes (timing, dose, formulation) often fix it.
Bottom line: This is the ideal path we aim for. If your journey looks different, it doesn’t mean treatment isn’t working we’ll adjust and keep going together. We will aim for small meaningful wins, measured in ways you can see. We will keep treatments safe and time limited, and we will stay curious about your gut, your patterns, and what helps you suffer less.
Key Message
Postprandial distress is a real, physical condition caused by nerve hypersensitivity in the gut. The problem lies in how brain and gut nerves process signals, not in your imagination. Normal tests don’t rule it out. Different treatments, including neuromodulating medications, diet, attention to healthy lifestyle and reassurance, are ways of resetting the system’s sensitivity. With the right strategies, most people improve or recover.
Neuromodulators for Gut Hypersensitivity
Peripheral agents
These act locally on the gut to improve motility and reduce spasms:
-
Prokinetics:
-
Domperidone, metoclopramide, mosapride, prucalopride → enhance stomach and intestinal movement, useful for fullness and delayed emptying.
-
-
Antispasmodics:
-
Peppermint oil, L-menthol → relax gut muscle; also act via κ-opioid receptor agonism and 5-HT₃ antagonism.
-
Mebeverine, hyoscine → reduce spasms and cramping.
-
-
Herbal therapies:
-
Iberogast → a multi-herbal extract (9 plants including bitter candytuft, chamomile, caraway, lemon balm). Acts as a prokinetic and spasmolytic; thought to reduce hypersensitivity.
-
Rikkunshito → a traditional Japanese Kampo formula made from eight herbs (including ginseng and ginger). May improve gastric accommodation and reduce early satiety.
-
Central agents
These work on the brain–gut axis to reduce pain sensitivity, improve sleep, and calm stress-related signalling:
-
Tricyclic antidepressants (TCAs): Amitriptyline, nortriptyline → first-line for gut pain hypersensitivity, especially with poor sleep.
-
SNRIs: Duloxetine → helpful where pain overlaps with anxiety or mood symptoms.
-
SSRIs: Sertraline → can be useful in IBS with constipation (IBS-C).
-
Gabapentinoids (α₂δ-ligands): Pregabalin, gabapentin → may reduce visceral hypersensitivity, bloating, and pain.